旋毛形线虫 旋毛虫 Trichinella spiralis
互联网
Trichinella spiralis 旋毛形线虫 旋毛虫
Trichinella spiralis(Owen, 1835), which exhibits the most unusual life cycle, is the smallest nematode parasite of humans and also is the most widespread and clinically important organisms in the world. T. spiralis is responsible for the disease known as trichinosis, trichiniasis, or trichinelliasis. It is common in carnivorous mammals, including pigs, rodents and humans, primarily on the circumboreal continents and is less common in tropical region. Incidence of infection is always higher than suspected because of the vagueness of symptoms, which usually suggests other conditions; more than 50 different disease have been diagnosed incorrectly as trichinosis.
Morphology

female

male
Adults: The male measure 1.4-1.6mm long and are more slender at the anterior than at the posterior end. A copulatory spicule is absent. Females are about twice the size of males, also tapering toward the anterior end. The vulva is located near the middle of the esophagus, which is about a third of the length of the body. The single uterus is filled with developing eggs in its posterior portion, whereas the anterior portion contains fully developed, hatched juveniles.
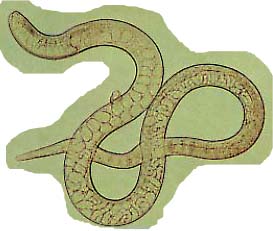
Cysts: The cysts encapsulates juveniles are spiral and located in the skeletal muscle.Although one worm per cyst is most common, up to seven have been observed in a single cyst within a single muscle cell.

肌肉切片

肌肉压片
Life Cycle
Ingest raw or poorly cooked: pork, bear, walrus, horse with viable larvae
Excyst, invade gut mucosa
4 larval stages
Adult, deposit larvae
Enter blood and lymph
Enter body tissue, encyst in diaphragm, larynx, tongue, jaws, neck, ribs, biceps
Become encapsulated
Cyst wall is from host IR
The larvae are viable for years; calcify
It really does happen that way:

Pathogenesis
The pathogenesis of Trichinella infection can be considered in three successive stages: penetration of adult females into the mucosa, migration of juveniles, and penetration and encystment in muscle cells.
First symptoms may appear between 12 hours and 2 days after ingestion of infected meat. Commonly, this phase is clinically inapparent because of low-grade infection or is misdiagnosed because of the vagueness of symptoms. When the gravid females penetrate the intestinal epithelium, they cause traumatic damage to the host tissues; they begin poisoning the host with their waste products, and they introduce enteric bacteria into the wounds they cause. These wounds result in intestinal inflammation and pain, with symptoms of food poisioning, such as nausea, vomiting, sweating, and diarrhea. Respiratory difficulties may occur, and red blotches erupt on the skin in some cases. This period usually terminates with facial edema and fever 5 to 7 days after the first symptoms.
During migration, the newborn juveniles damage blood vessels, resulting in localized edema, particularly in the face and hands. Wandering juveniles may also cause pneumonia, pleurisy, encephalitis, meningitis, nephritis, deafness, peritonitis, brain or eye damage, and subconjunctival or sublingual hemorrhage. Death resulting form myocarditis (inflammation of the heart muscle)may occur at this stage. Although the juveniles do not stay in the heart, they migrate through its muscle, causing local areas of necrosis and infiltration of leukocytes.
By the tenth day after the first symptoms appear, the juveniles begin penetration of muscle fibers. Attendant symptoms are again varied and vague: intense muscle pain, difficulty in breathing or swallowing, swelling of masseter muscles (occasionally leading to a misdiagnosis of mumps), weakening of pulse and blood pressure, heart damage, and various nervous disorders, including hallucination. Extreme eosinophilia is common but may not be present in even severe cases. Death is usually caused by heart failure, respiratory complications, toxemia, or kidney malfuction.
Diagnosis and treatment
Most cases of trichinosis, particularly subclinical cases, go undetected. Even extreme infection of 1,000 juveniles or more per gram of body weight may go undetected if the attending physician does not suspect trichinosis. Routine examination rarely detect juveniles in feces, blood, milk, or other secretions. Although muscle biopsy is seldom employed, it remains an accurate diagnostic if trichinosis is suspected. Pressing the tissue between glass plates and examining it under low-power-microscopy is useful, although digestion of the muscle in artificial gastric enzymes for several hours provides a much more reliable diagnostic technique. Xenodiagnosis, feeding suspected biopsies to laboratory rats, may be employed. Several immunodiagnostic techniques have been developed, none of which is 100% effective but which are useful nonetheless.
images:



No really satisfactory treatment for trichinosis is known. Treatment is basically that of relieving the symptoms by use of analgesics and corticosteroids. Purgs during the initial symptoms may dislodge females that have not yet begun penetrating the intestinal epithelium. thiabendazole has been khown effective in experimental animals, but results in clinical cases have been variable.
Despite and immense amount of research, trichinosis remains an important disease of humans, one that has the potential of striking anyone, anywhere. One hopeful note: for unknown reasons, the incidence of infection has slowly but steadily declined throughout the world.
Epidemiology
The incidence of infection is always higher than suspected because of the vagueness of symptoms, which usually suggests other conditions. trichinosis has a cosmopolitan distribution but is more important as an infection of man in Europe and the United States than it is in the tropics and orient. In China, heman trichinosis have been reported in Tibet, Yunnan, Henan, and the northest part of China.
Most wild and domestic mammals are susceptible to infection. Fatal cases of trichinosis are common among those who eat inadequately cooked or frozen bear, wild pig, cat, dog, or walrus meat. Any wild mammal may be a source of infection. Urban trichinosis is epidemiologically more important to humans because of the close relationship among rats, pigs, and peole. Infected pork is our most common source of infection. Pigs become infected by eating offal or trichinous meat in garbage. It is usually concluded that garbage containing raw pork scraps is the usual source of infection for pigs. The importance of cooking pork thoroughly before it is eaten cannot be overstated. A roast or other piece of solid meat is safe when all traces of pink have disappeard. freezing at -15℃ for 20 days destroys all parasites, at least in the temperate zone strain.
Survivors of trichinosis have varying degree of immunity to further infection.